





Demographic data
In total, 490 patients meeting Rome III criteria for IBS-D were enrolled in this study, with an average age of 41.6 ± 11.2 years. There were 299 male patients (61.0%) and 191 female patients (39.0%). Female patients were older and had lower body mass index (BMI) than male patients. The percent of education with college and above in female patients was lower than male patients (Table 1). There were no significant differences in family economic status, marriage status, the average IBS disease course (all P > 0.05).
Characteristics of bowel symptoms
More female patients reported having defecatory abdominal pain than male patients (84.3% vs. 74.9%, P = 0.014), while more male patients reported defecatory abdominal discomfort than female patients (39.8% vs. 26.7%, P = 0.003). The locations of abdominal pain/discomfort were mainly in the lower abdomen followed by the umbilical region, there was no significant difference in distribution of abdominal pain/discomfort locations (P > 0.05, Fig. 1A and B). More patients in the female group reported severe abdominal pain/discomfort than those in the male group (17.8% vs. 12.4%, P = 0.013, Fig. 1C and D). There were no significant differences in symptom frequency (P = 0.490, Fig. 1E and F) and the prevalence of ordinary abdominal pain or/and discomfort between the two groups (47.8% vs. 41.4%, P = 0.161).
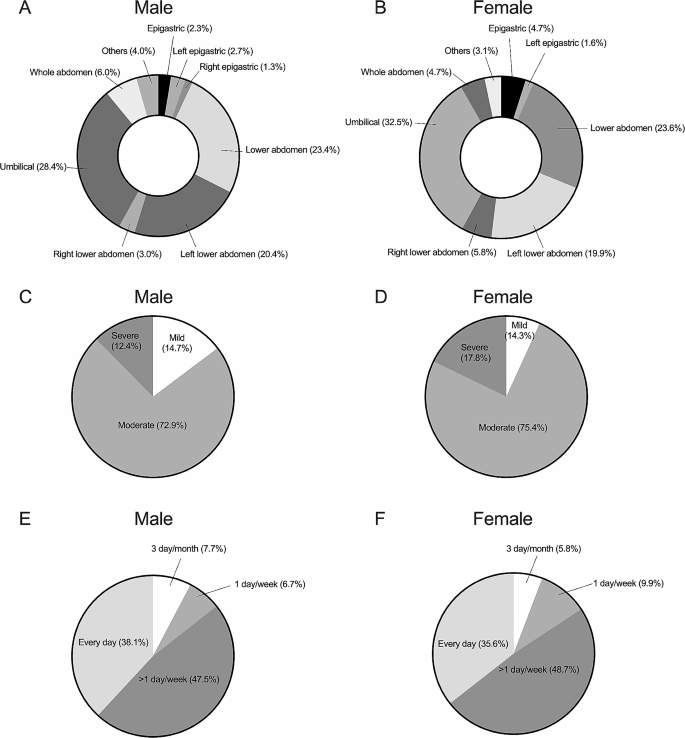
Comparison of the location, severity and frequency of defecatory abdominal pain/discomfort between male and female patients with irritable bowel syndrome predominant with diarrhea. A, B, the percentages of locations of defecatory abdominal pain/discomfort; C, D, the percentages of severity of defecatory abdominal pain/discomfort; E, F, the percentages of frequency of defecatory abdominal pain/discomfort. Female patients reported higher severe abdominal pain/discomfort than male patients, others were not significantly different
There were no significant differences in average bowel movements (Fig. 2A) and stool form during symptom onset period (Fig. 2B) between the two groups. The IBS symptom score of female patients was higher than male patients (9.7 ± 1.7 vs. 9.4 ± 1.4, P = 0.025), which indicated more severe symptoms for females.
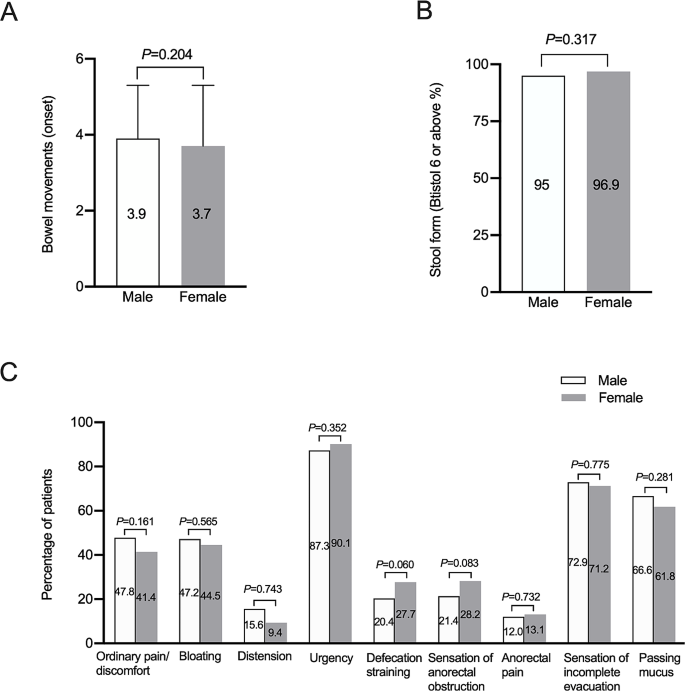
Comparison of abdominal symptoms and defecatory symptoms between male and female patients with irritable bowel syndrome predominant with diarrhea. A, comparison of bowel movements during symptom onset; B, comparison of the percentage of Bristol stool form 6 or above during symptom onset; C, comparison of other abdominal symptoms and defecatory symptoms
The female and male patients had similar prevalence of abdominal bloating, abdominal distension, urgency, defecation straining, sensation of anorectal obstruction, anorectal pain, sensation of incomplete evacuation (Fig. 2C).
Extra-intestinal symptoms
There were no significant differences in the prevalence of GERD or FD between the two groups (all P > 0.05), but the prevalence of food regurgitation was higher in male group (Table 2). More patients in the male group reported frequent micturition than female group (Table 2).
Comorbid anxiety and depression state
More female patients reported having sleep disorder in the past 3 months than males (Fig. 3A). Female patients reported higher incidence of mental stimulation history (Fig. 3A). There was no significant difference of self-reported abuse history (Fig. 3A). The scores of HAMA and HAMD were significant higher in female group than male group (Fig. 3B). The prevalence of comorbid anxiety state as well as moderate-to-severe anxiety state and the prevalence of comorbid depression state including mild and moderate-to-severe depression state were higher in female group than male group (all P < 0.05, Fig. 3C and D). Female patients were more likely to have anxiety and depression state at the same time (33.0% vs. 18.4%, P < 0.001).
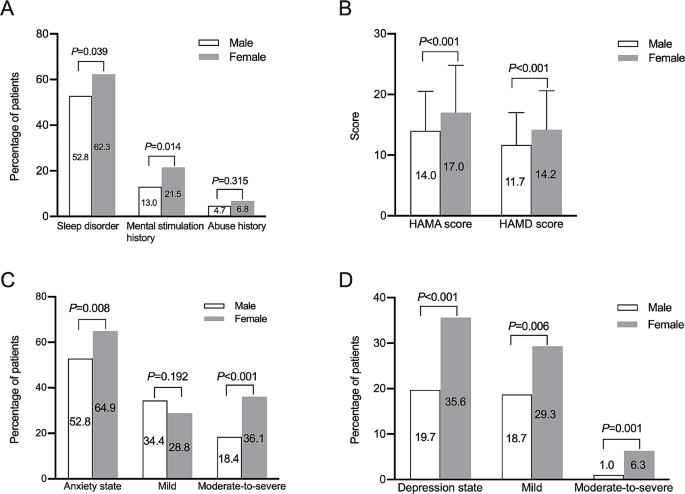
Comparison of psychological disorders between male and female patients with irritable bowel syndrome predominant with diarrhea. A, comparison of the percentages of sleep disorder, mental stimulation history and abuse history; B, comparison of HAMA and HAMD scores; C, comparison of the prevalence of anxiety; D, comparison of the prevalence of depression
More female patients reported their worsening bowel symptoms were related with their terrible emotion than males (49.7% vs. 35.8%, P = 0.002), but similar percentages of patients reported the relation of worsening bowel symptoms with sleep disorder in the two groups (18.8% in females and 17.4% in males, P = 0.682).
Among the patients with mild-to-moderate abdominal pain/discomfort, females had higher prevalence of comorbid anxiety state (72.8% vs. 57.0%, P = 0.004), moderate-to-severe anxiety state (44% vs. 19.6%, P < 0.001) and depression state (41.6% vs. 22.0%, P < 0.001) than males. Among the patients with mild-to-moderate symptoms (IBS symptom score ≤ 10), females had higher prevalence of comorbid anxiety state (64.9% vs. 53.3%, P = 0.030), moderate-to-severe anxiety state (38.1% vs. 18.3%, P < 0.001) and moderate-to-severe depression state (7.5% vs. 1.25%, P = 0.024) than male patients.
Among the patients with severe abdominal pain/discomfort, there were no significant differences of the prevalence of anxiety state (75.7% vs. 67.6%, P = 0.452) or depression state (24.3% vs. 29.4%, P = 0.629) between males and females. In patients with severe symptoms (IBS symptom score > 10), females had higher prevalence of comorbid depression state than males (40.4% vs. 16.9%, P = 0.005), while there was no significant difference of anxiety state between the two groups (P > 0.05).
In male patients, IBS symptom score had a tendency to positively correlated with HAMD score (r = 0.113, P = 0.05), but was not correlated with HAMA score (r = 0.058, P = 0.314). In female patients, IBS symptom score was not correlated with HAMD (r = 0.103, P = 0.156) or HAMA score (r = 0.070, P = 0.334).
IBS-QOL score
The IBS-QOL score of patients with IBS-D showed an obvious decrease with 75.1 ± 16.8 in the male group, 70.2 ± 20.4 in the female group while comparing to the mean total score in healthy Chinese subjects (95.50 ± 6.73 with the scores on each of the eight domains being ≥ 90.00) [20]. The IBS-QOL score of female patients was significantly lower than male patients especially in the domains of food avoidance, dysphoria, interference with activity, social reaction and body image (Table 3, all P < 0.05).
Although bowel symptoms, comorbid anxiety and depression and IBS-QOL score were different between male and female patients, their HAMA score, HAMD score and IBS symptoms score were both negatively correlated with IBS-QOL score (Fig. 4).
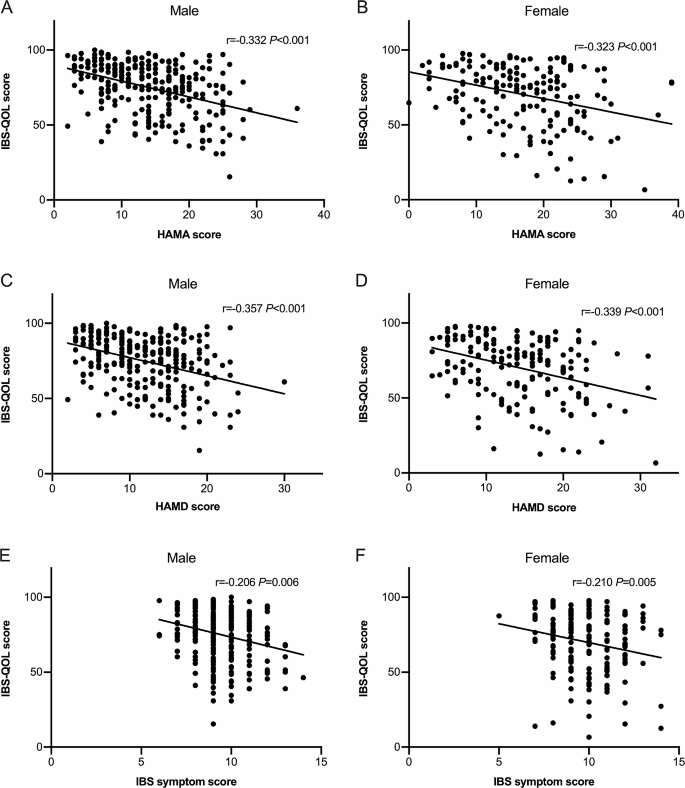
The correlation of anxiety, depression, IBS symptom with IBS-QOL score in male and female patients. The HAMA score (A, B), HAMD score (C, D), IBS symptoms score (E, F) were negatively correlated with IBS-QOL score
Dietary habits and coping behaviors
The proportion of selecting staple food or dish food as dominant or equivalent in both were similar between male and female patients. Of 52.9% female patients reported vegetables were their dominant components of dish food, and 24.1% male patients reported meat was their dominant components of dish food (Table 4). More male patients reported they often consume the greasy food than females. More than half of patients in the two groups took dietary modifications to relieve bowel symptoms, male patients reported higher response rate than females (Table 4).
Healthcare-seeking behaviors
Female patients reported more consultations per year in the whole disease course than male patients for IBS (Table 5). More than half of patients in the two groups chose to visit tertiary hospitals. There were no significant differences between the two groups in the average number of consultations in the last year, colonoscopies in the whole disease course and intermittent and long-term medication use in the last year (all P > 0.05). The overall satisfaction rate (including complete satisfaction and satisfaction) with medical care and average medical cost per year showed no significant differences between the two groups (all P > 0.05) (Table 5).
link
More Stories
Pediatric Gastroenterology – MU Health Care
Leading Gastroenterology Hospitals Advancing Digestive Care in India
Mobile ‘Endoscopy on Wheels’ Delivers Lifesaving Gastrointestinal Care